3D Compression Technology
3D compression technology combines both cardiac and thoracic pump theory. This patent is owned by Weil Institute of Critical Care Medicine (Fig a). Special Features – High Efficiency, Less Traumatic.
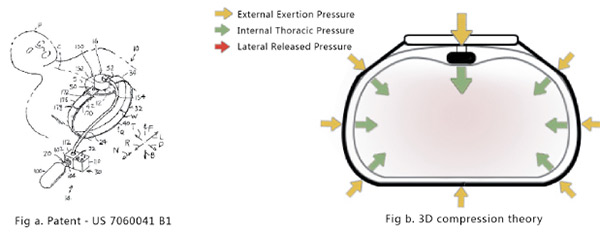
HIGH EFFICIENCY- In additional to vertical chest compression between the sternum (chest bone) and the spine, the torso restraint is placed underneath and around the patient to firmly secure the compressor onto the patient which will compress the whole chest cavity to circulate blood instantly. This will create a highly effective three dimensional chest compression.(Fig b.)
A report published by the Weil Institute Critical Care Medicine research team comparing 3D chest compression technology to traditional CPR compression method. It showed that within an experiment setting, half the compression depth delivered by 3D chest compression technology can effectively increase the coronary perfusion pressure (CPP) equal to full compression depth normally delivered by traditional compression technology . This technology is non-invasive and is the closest method to resemble the heart’s 3D pumping action.
| Experiment Item | Other Brand
|
Weil MCC |
Explanation |
|---|---|---|---|
| Effect on Coronary Perfusion Pressure and chest compression depth | 12-20 mmHg 5.3-6.1 cm |
14-50 mmHg 3.0-3.5 cm |
50% compression depth delivered by Weil Mini Chest Compressor has the same effect as 100% compression depth delivered by other band |
| Intrathoracic Positive Pressure | 10 mmHg | 31 mmHg | Favour blood circulation |
| Intrathoracic Negative Pressure | -3 mmHg | -10 mmHg | Favour blood perfusion |
| Chest Compression Time | 11 minutes | 5 minutes | Fast recovery |
| Number of shock before ROSC | 9.8 times | 1 times | Less electrical shock |
LESS TRAUMATIC - According to research studies, 3D chest compression technology can shorten the compression cycle and the number of electrical shocks. Rib fractures and neuro deficit can also be minimized.
| Experiment Item | Other Brand |
Weil MCC | Explanation |
|---|---|---|---|
| Number of broken Ribs | Average 2.75 | Nil | Less to none complication and injurt |
| Carotid Artery Blood Flow | 23.5 mL/min | 42.3 mL/min | Better blood perfusion to the brain |
| Neurobehavioral Assessment Scale (NAS) | 35.6 | 88.1 | Better neuro recovery |
| Neurobehavioral Assessment Scale (NAS) | 47.5 | 97.5 | Better Neuro recovery |
Development Trends of Mechanical Chest Compressor
There is an urgent need for high quality CPR in emergency medicine. Since there are limitations in manual CPR, there are high demands for new compression technology to improve blood flow while performing CPR.
The main objective is to revive the patient and to improve blood flow to the heart and brain.
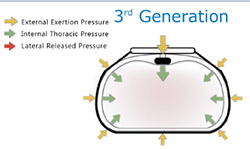 |
3rd Generation Mechanical Chest Compression Technology: 3D CompressionTheory : Cardiac and Thoracic Pump Theory. “3D Compression” - 100% chest cavity is enclosed with the torso restraint. In addition to multi-points compression, whole chest cavity is compressed to simulate heart pump function. |
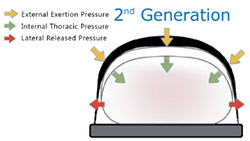 |
2nd Generation Mechanical Chest Compression Technology: Load Distributing Band CompressionTheory : Thoracic Pump Theory. “Load Distributing Band Compression” - Breakthrough from the Single Point Compression, squeezes a wide area of the chest (50%) multi-point compression spreading out the force of compressions. |
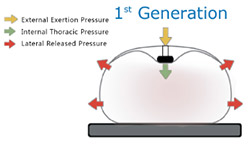 |
1st Generation Mechanical Chest Compression Technology: Single Point CompressionTheory : Cardiac Pump Theory. “Single Point Compression” - Simulate hands-only compression, single point compression, high impact force. |
DATA SOURCES: *Data Source: Wei Chen, MD, PhD; Yinlun Weng, MD, PhD; Xiaobo Wu, BME; Shijie Sun, MD, FCCM;Joe Bisera, MSEE;Max Harry Weil, MD,PhD, MCCM;Wanchun Tang,MD, MCCM. The effects of a newly developed miniaturized mechanical chest compressor on outcomes of cardiopulmonary resuscitation in a procine model, Crit. Care Med 2012 Vol 40 No.11